Post-Tubal Ligation Syndrome (PTLS)
Post-Tubal Ligation Syndrome (PTLS) is a term used to describe a collection of symptoms that some women report after undergoing tubal ligation, commonly referred to as “getting your tubes tied.” While tubal ligation is widely considered a safe and effective permanent contraceptive method, PTLS remains a controversial topic within the medical community due to limited high-quality evidence confirming it as a distinct clinical diagnosis.
This article explores what PTLS is, the proposed mechanisms, reported symptoms, diagnostic considerations, and current perspectives in medical research.
What Is Tubal Ligation?
Tubal ligation is a surgical sterilization procedure in which the fallopian tubes are cut, sealed, clipped, or cauterized to prevent sperm from reaching the ovum. It may be performed:
Postpartum (often immediately after delivery)
During cesarean section
As an interval laparoscopic procedure
Concurrently with other pelvic surgeries
Tubal ligation does not directly remove or alter the ovaries or uterus and, in theory, should not affect hormonal function.
What Is Post-Tubal Ligation Syndrome?
PTLS is described as a set of physical and psychological symptoms that develop after tubal sterilization. The term is not formally recognized by major organizations such as the American College of Obstetricians and Gynecologists (ACOG) or the World Health Organization (WHO) as a defined medical condition. However, patient-reported experiences have led to ongoing discussion in gynecologic practice.
Some clinicians prefer to frame symptoms within broader diagnostic categories rather than labeling them as PTLS.
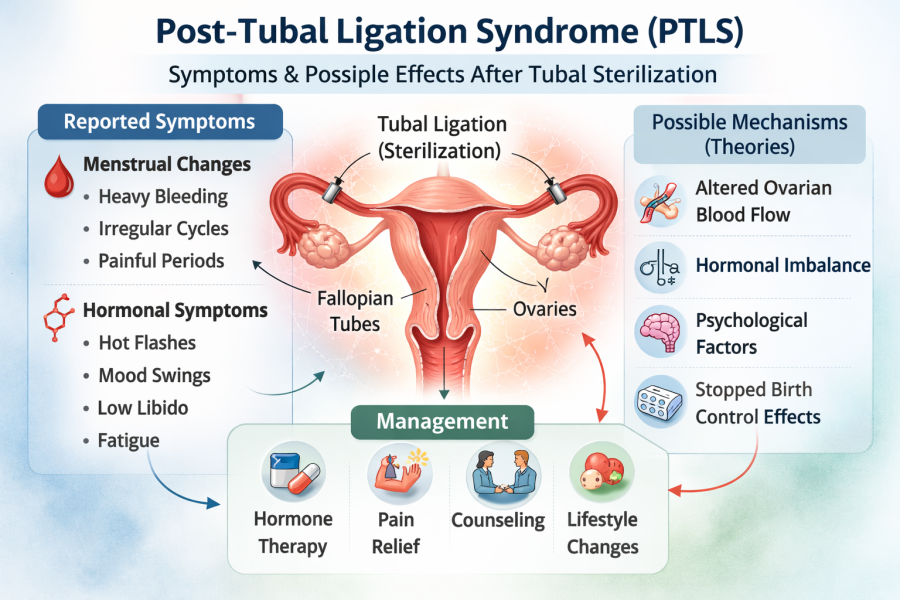
Reported Symptoms of PTLS
Women who believe they are experiencing PTLS commonly report:
Menstrual Changes
Heavier menstrual bleeding (menorrhagia)
Irregular cycles
Increased dysmenorrhea
Premenstrual syndrome (PMS) worsening
Hormonal Symptoms
Hot flashes
Night sweats
Mood instability
Decreased libido
Fatigue
Pelvic Pain
Chronic pelvic pain
Dyspareunia
Psychological Symptoms
Anxiety
Depression
Irritability
It is important to note that many of these symptoms overlap with natural aging, perimenopause, thyroid disorders, stress-related conditions, or preexisting gynecologic disorders.
Proposed Mechanisms
Although definitive evidence is lacking, several theories have been proposed:
1. Altered Ovarian Blood Flow
Some hypothesize that tubal ligation may disrupt blood supply to the ovaries through damage to the mesosalpinx, potentially affecting ovarian hormone production.
However, Doppler and hormonal studies have generally shown no consistent long-term impairment in ovarian function following sterilization.
2. Hormonal Imbalance
Anecdotal reports suggest estrogen and progesterone fluctuations post-procedure. Most controlled studies, however, have not demonstrated significant endocrine differences compared to non-sterilized women.
3. Psychological Factors
In some cases, regret after sterilization or life changes may contribute to psychological distress, which can amplify perceived physical symptoms.
4. Discontinuation of Hormonal Contraception
Many women stop hormonal birth control after tubal ligation. Symptoms previously suppressed by contraceptives (e.g., heavy bleeding, PMS) may then emerge and be attributed to the procedure itself.
Current Evidence and Research
Large cohort studies have generally not supported a consistent syndrome directly caused by tubal ligation. Research indicates:
No strong association with premature ovarian failure
No consistent evidence of accelerated menopause
No reliable hormonal pattern unique to post-sterilization patients
That said, individual variation in symptom perception and response to surgery should not be dismissed. Patient-centered care requires acknowledging symptoms while evaluating alternative explanations.
Differential Diagnosis
When patients present with symptoms attributed to PTLS, clinicians should consider:
Perimenopause
Polycystic ovary syndrome (PCOS)
Thyroid dysfunction
Endometriosis
Adenomyosis
Uterine fibroids
Chronic pelvic inflammatory disease
Depression or anxiety disorders
A thorough history, hormonal evaluation, pelvic imaging, and appropriate laboratory testing are recommended before attributing symptoms to sterilization.
Management Strategies
Since PTLS is not a formally established diagnosis, treatment is symptom-based:
Hormonal therapy for menstrual irregularities
NSAIDs or other analgesics for pelvic pain
Endometrial ablation for heavy bleeding (in selected cases)
Psychological counseling when emotional distress is present
Lifestyle modifications, including weight management, sleep hygiene, and stress reduction
In rare cases, patients may request tubal reversal or hysterectomy; however, evidence that these procedures reliably resolve symptoms is limited.
Counseling and Informed Consent
Preoperative counseling is critical. Patients considering tubal ligation should be informed that:
It is intended to be permanent.
It does not regulate menstrual cycles.
Stopping hormonal contraception may change bleeding patterns.
Current evidence does not support a well-defined post-tubal ligation syndrome.
Clear expectations may reduce postoperative dissatisfaction and perceived complications.
Clinical Perspective
From an evidence-based standpoint, PTLS remains a debated entity. While patient-reported symptoms are real and deserve evaluation, high-quality data have not confirmed a distinct physiological syndrome directly caused by tubal ligation.
Clinicians should approach concerns with empathy, avoid dismissing symptoms, and conduct comprehensive assessments to identify treatable conditions.
Conclusion
Post-Tubal Ligation Syndrome (PTLS) is a controversial and not formally recognized diagnosis describing symptoms some women experience after sterilization. Although current research does not strongly support a direct causal relationship between tubal ligation and long-term hormonal disruption, individualized care and careful evaluation remain essential.
For medical professionals, the key lies in balanced counseling, thorough diagnostic workup, and evidence-based management tailored to each patient’s presentation.